
Anti-acid Medications & Vitamin B12 Absorption
A brief note before you get started reading through this one –
Medications like these may be best prescribed as short term interventions in addition to lifestyle (dietary/exercise/sleep/stress) adjustments for chronic gastric acid complications such as acid reflux or GERD. Food is not medicine and should never be used in replacement of a physician prescribed medication unless directed to do so by your doctor. The issue is that there was limited research and evidence supporting my discussion in this post when doctors were prescribing them for long term, chronic gastric acid complications. This a complex, and multifaceted issue and is very dependent upon potential underlying complications and the chronicity of the situation, as most health concerns and conditions are. Therefore, you should always consult your physician if you have any concerns or questions about your current intervention.
Long-term use of antacids, histamine-2 receptor antagonists (H2 blockers or H2RAs), and proton-pump inhibitors (PPIs), meant to address acid-related conditions in humans, are associated with adverse neurological, gastrointestinal, and hematological conditions. Complications include depression, dementia, anemia, and neuropathy, all symptoms that are associated with the inhibition of vitamin B12 absorption.1-4
Here are some examples of common over-the-counter and prescribed antacid medications that you may be familiar with:
| Antacid | H2 Blockers | PPIs |
| Tums | Axid | Nexium |
| Alka-Seltzer | Tagament | Prilosec |
| Rolaids | Pepcid | Prevacid |
| Pepto-Bismol | Zantac | Protonix |
| Gaviscon | Dexilant | |
| Mylanta | Aciphex | |
| Zegerid |
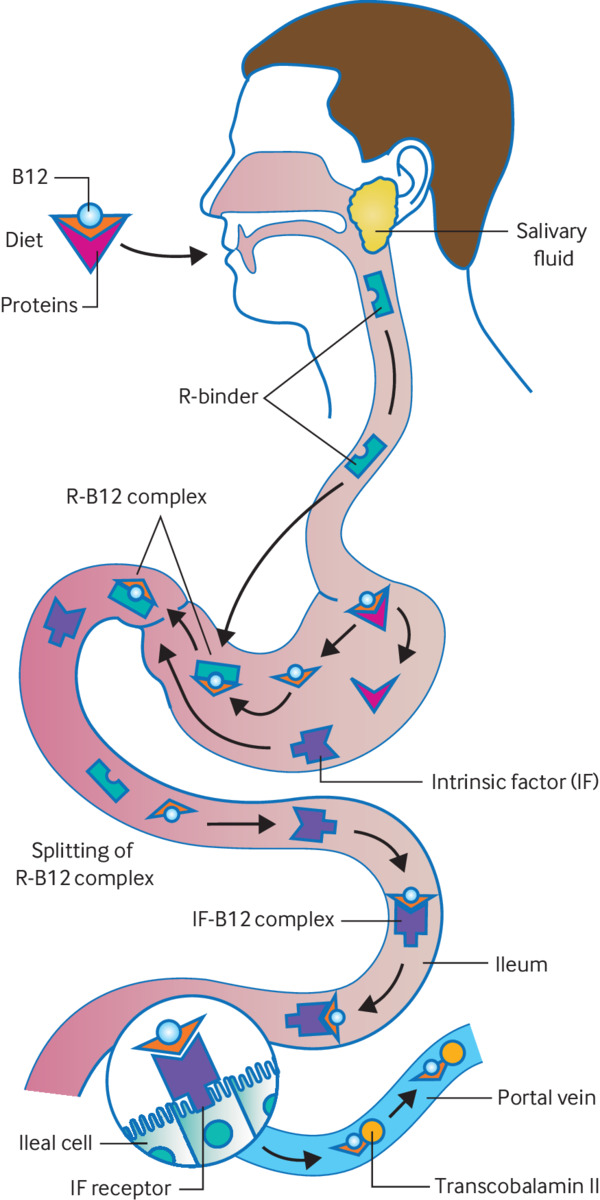
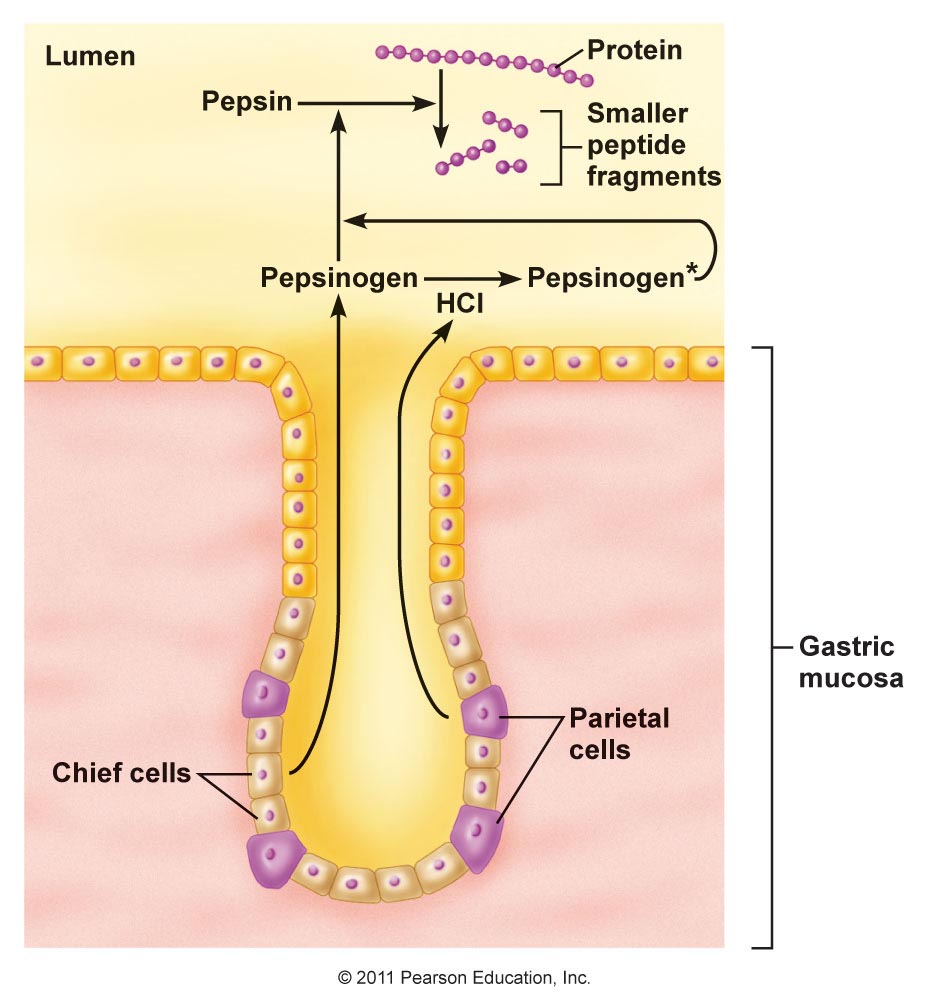
Vitamin B12 is released from animal protein bonds in the highly acidic environment of the human stomach, where it is then bound to R-factor (haptocorrin) and transported to the duodenum for further absorption by intrinsic factor (IF) in the small intestine.1,5 The diagram below illustrates how protein is metabolized throughout digestion.
Hydrochloric acid (HCl, not shown in above diagram), released by the parietal cells in the stomach, is required for the activation of pepsinogen to pepsin, a protease released by chief cells in the stomach.
Over the counter and prescribed antacid medications alter the acidic pH by neutralizing stomach acid after it has been secreted, increasing alkalinity by inhibiting parietal cell production of HCl and Intrinsic Factor (IF), later diminishing the rate of release and absorption of B12 throughout chemical digestion in the small intestine.1,2
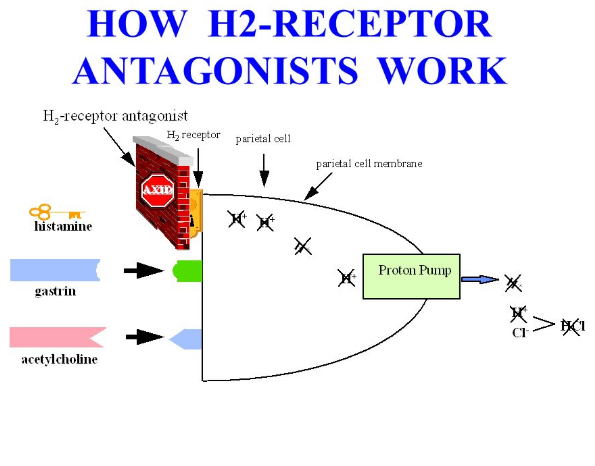
H2 Receptor Antagonists (H2RAs) inhibit the binding of histamine-2 to histamine-2 receptors on the parietal cells, therefore inhibiting the hydrogen/potassium pumps (H+K+-ATPase) from pumping hydrogen (H+) molecules into the lumen of the stomach where it will react with Cl- to create HCl. This is illustrated below.
Prescribed Proton Pump Inhibitors allow histamine-2 to bind with the parietal cell but blocks the H+K+-ATPase function of releasing hydrogen into the lumen, therefore inhibiting HCl production. 29% of long-term PPI users are vitamin B12 deficient and 95% of vitamin B12 deficiency cases are highly associated with malabsorption.5,6

Hematological and neurological conditions often present together with vitamin B12 deficiency; however, anemias tend to be earlier indicators with neurological symptoms to come later.7,8 Without adequate vitamin B12, homocysteine cannot be converted to methionine. This manifests megaloblastic anemia and the accumulation of homocysteine. Manifestations of homocysteine accumulation and methylmalonic acid (MMA) can also cause damage to the myelin of nerve cells. Without adequate vitamin B12, MMA cannot be converted into succinyl-CoA, a substrate required in the citric acid cycle contributing to energy production in the human body. Expected neurological symptoms of long-term vitamin B12 deficiency include myelopathy, neuropathy, dementia, and depression.7-9
References:
1. Miller JW. Proton Pump Inhibitors, H2-Receptor Antagonists, Metformin, and Vitamin B-12 Deficiency: Clinical Implications. Adv Nutr. 2018;9(4):511S–518S. doi:10.1093/advances/nmy023
2. Brusewicz J. Neuropathy & Long-term PPI Use: A Case Study. https://ndnr.com/gastrointestinal/neuropathy-long-term-ppi-use-a-case-study/. Published January 11, 2016. Accessed January 8, 2019.
3. Novotny M, Klimova B, Valis M. PPI Long Term Use: Risk of Neurological Adverse Events? Front Neurol. 2019;9:1142. doi:10.3389/fneur.2018.01142
4. Makunts T, Alpatty S, Lee KC, Atayee RS, Abagyan R. Proton-pump inhibitor use is associated with a broad spectrum of neurological adverse events including impaired hearing, vision, and memory. Sci Rep. 2019;9(1):17280. doi:10.1038/s41598-019-53622-3
5. Pizzorno JE, Katzinger J. Clinical Pathophysiology: A Functional Perspective. Coquitlam, BC Canada: Mind Publishing Inc; 2012.
6. Neiman DC. Nutritional Assessment. 7th ed. New York, New York: McGraw-Hill Education; 2019.
7. Ralapanawa DM, Jayawickreme KP, Ekanayake EM, Jayalath WA. B12 deficiency with neurological manifestations in the absence of anaemia. BMC Res Notes. 2015;8:458. doi:10.1186/s13104-015-1437-9
8. Ekabe CJ, Kehbila J, Abanda MH, Kadia BM, Sama CB, Monekosso GL. Vitamin B12 deficiency neuropathy; a rare diagnosis in young adults: a case report. BMC Res Notes. 2017;10(1):72. doi:10.1186/s13104-017-2393-3
9. Ankar A, Kumar A. Vitamin B12 Deficiency (Cobalamin). https://www.ncbi.nlm.nih.gov/books/NBK441923/. Updated January 11, 2019. Accessed January 8, 2019.
Be the first to comment